To get an idea of what your shoulder does take your right hand and try the following: scratch your nose; scratch your left bum cheek; scratch your belly; give a high-five; do your best karate kid impression and wax on wax off; pull a curtain across from left to right and right to left; take your hand up behind your back with the palm facing out; take your hand down behind your head with the palm facing in. Your shoulder must accommodate this huge range of movement safely, smoothly and whilst remaining stable. It’s the potential conflict between mobility and stability that contributes to some of the shoulder impingement issues that you can read about here.
Risk factors / Causes:
The most common cause of shoulder dislocation occurs when the arm is held away from the body during a fall or tackle. We physios refer to this vulnerable position as the stop sign position – arm at 90 degrees to the body, hand and palm facing forwards. The arm is forced backwards and the trunk forwards resulting in the shoulder popping out of its socket. The first time shoulder dislocation typically causes widespread damage to the bony, muscle and connective tissue of the joint (the glenohumeral joint).
Occasionally we see patients who have had multiple dislocations resulting in an unstable shoulder that can pop in and out (sublux) with little or no pain or loss of function. This type of instability can also occur due to repetitive stress of the joint as seen in swimmers, golfers and volleyballers. It is also evident in people with genetically hypermobile joints.
Management:
The rehabilitation options for a dislocated shoulder are similar to those for the ACL. If you’re a footballer, a surfer a gymnast or bricklayer reliant upon a stable joint throughout the entire range of movement then off to the surgeon you go. Even if you’re none of these, surgery may be required to deal with the painful symptoms emanating from the widespread tissue damage often seen post dislocation.
Irrespective of the management pathway the primary goals are to restore range, stability and higher-level sport or work-specific functioning.
Our arms and legs are often referred to as appendages and unfortunately this is how many shoulder rehab plans are designed, forgetting that the arm and shoulder function in conjunction with the joints, muscles, fascia and connective tissue of the chest, back, butt and legs. Here at Construct Health we rehabilitate the entire body, stabilising the shoulder in conjunction with reconnecting and re-establishing its dynamic relationship with the entire body.
If you’re goal is to rebuild a dynamic highly functioning shoulder after dislocation then contact us and come and see one of our highly qualified physios today [ Click here to Request an Appointment ]
Rotator Cuff (RC) Tear
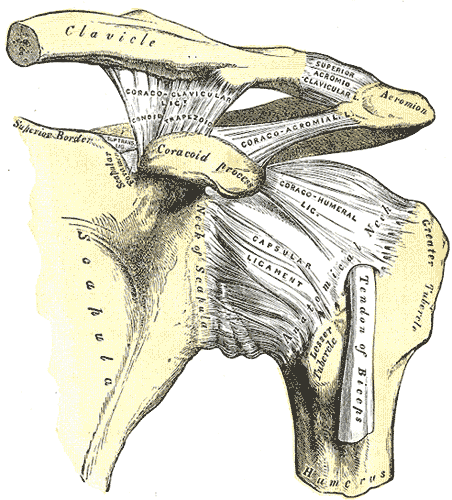
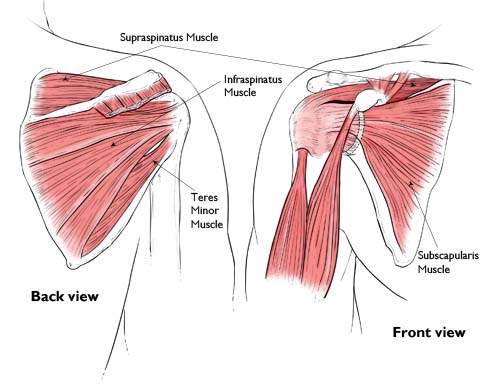
The shoulder is stabilised by the combined action of a passive osseo ligamentous system (fancy physio speak for bone, ligament, fascial and fibrous tissue) and an active musculotendinous system. The musculotendinous system is made of four small muscles (supraspinatus, subscapularis, infraspinatus and teres minor) collectively known as the rotator cuff. These muscles work in combination to move and stabilise the shoulder joint during arm movement. A big part of their function is to maintain the head of the humerus centred within the joint. Dysfunctions in this system can lead to shoulder impingement syndrome which you can read about here.
Tears within the rotator cuff tendons usually occur as a result of ongoing microtrauma or age-related degenerative changes. Acute tears, whilst less common, are generally related to heavy, high-speed loading such as grabbing a railing to stop a fall.
Rotator Cuff tears are either full or partial thickness. The greater the tear usually the worse the symptoms of pain and loss of shoulder function.
Risk Factors / Causes:
The risk factors for degenerative rotator cuff tears are very similar to those for impingement syndrome – poor shoulder, cervical and thoracic biomechanics, poor posture and repetitive overhead work. Father time also has a big role to play, with significant rates of degenerative tears evident as we enter our 50’s and beyond. Research has shown that tears exist even in absence of pain or loss of function.
Here at Construct Health we often see traumatic rotator cuff tears as the result of slips or falls down steps or ladders. The injured person has attempted to stop the fall by reaching out for a hand rail and in the process suffer a RC tear.
Management:
Minor cuff tears typically respond very well to a well-designed rehabilitation programmed aimed at restoring strength; scapulothoracic and scapulohumeral rhythm; and improving posture.
Surgery is sometimes called for to restore function or manage symptoms following a cuff tear. The surgery may be to stitch the tendon(s) back to together; to increase the size of the joint to reduce tendon friction and irritation; remove bony spurs and damaged tissue; or a combination of all of the above. Once surgery is complete the patient follows the same rehabilitation pathway as the non-surgically managed patient.
As with all of our patients, we aim to return the individual to their pre-injury level of work or sporting function. This may be through Pilates or home or gym-based exercise to improve muscular strength, endurance and power. We will often undertake a workplace visit to look at work practices; workstation set-up; job and task rotation; and all factors that contribute to either the original injury or the potential for reinjury.
If you’re goal is to rebuild a dynamic highly functioning shoulder following a rotator cuff repair or injury then contact us and come and see one of our highly qualified physios today [ Click here to Request an Appointment ]
AC Joint Disruption/sprain
The AC joint is the joint on the top of the shoulder where the collarbone (“C” for clavicle) and the acromion (“A” for acromion – part of the scapula or shoulder blade for the non-Latin speakers amongst us) join. Injury to this joint is fairly common following a fall onto or blow to the point of the shoulder or a fall onto the outstretched hand (quaintly termed a FOOSH). The tell-tail sign of significant AC joint injury is a “step” deformity on the top of the shoulder and pain reaching across the body.
Risk Factors / Causes:
As stated above this injury occurs either through a FOOSH or a blow to or fall onto the point of the shoulder resulting in damage to the ligaments that hold the collarbone and shoulder blade together. We physios grade ligamentous injury as Grade 1 – minor tissue damage with little loss of function; Grade 2 – moderate tissue damage with a concomitant increase in ligament stretch or laxity; or Grade 3 – complete rupture of the ligament(s) with significant joint changes.
Management:
Patients with minor AC joint injuries will start to feel better in a few days, whilst those with significant joint disruption may experience pain and dysfunction for up to six weeks.
The goal of physio with an AC joint injury is to restore normal pain-free movement. We focus upon lengthening muscles; mobilising stiff joints; and improving posture and movement patterns. As AC joint injuries are common in contact sports we are often called upon to perform fitness tests to see if an athlete can be “cleared” to safely return to their sport.
If you’re goal is to rebuild a dynamic highly functioning shoulder following an AC joint injury then contact us and come and see one of our highly qualified physios today [ Click here to Request an Appointment ]
Chronic
Shoulder Impingement
We’ve already discussed how the shoulder has to move a lot and remain stable (click here – to find out more about shoulder range and shoulder dislocation). When this balance is out of kilter we tend to get an impingement syndrome. Essentially the tendons of the dynamic stabiliser muscles of the shoulder, known collectively as the rotator cuff, rub against and get pinched between the bony and connective tissues of the shoulder joint. This rubbing and pinching sets in train an inflammatory process resulting in pain and restricted movement.
Risk Factors / Causes:
Very occasionally an impingement syndrome can occur as the result of a traumatic injury, but it usually presents in response to repetitive overhead arm movements.
Now lots of people perform repetitive overhead movements at work or sport and never develop impingement symptoms, so what puts some at risk and not others? It would seem that some people have genetically “smaller” spaces within the shoulder predisposing the rotator cuff tendons to irritation – note to self: pick better parents next time. Narrowing of the spaces within the shoulder is also more common as we age due to the growth of osteoarthritic bony spurs. At the other end of the spectrum are the “loose” shouldered folk who’ve had previous dislocations or whose sport or work has caused overstretching of the shoulder connective tissue. Combine this tissue laxity with poor posture and you get a shoulder that doesn’t “sit” as it should thus leading to the movement-related impingement.
Management:
When impingement is the result of a dynamic instability these folk may require surgery to repair the shoulder. Surgery is also used where significant degenerative changes are contributing to the symptoms and in cases where congenitally “narrow” spaces make conservative management unlikely to resolve the condition. Corticosteroid injections are also frequently used to settle bursa and tendon (-sheath) inflammation.
In most cases we aim to conservatively manage the painful symptoms and work on regaining range of movement, strength and movement control. In physio-world the way in which the shoulder blade and arm move together is referred to as scapulohumeral rhythm. Restoration of normal rhythm, particularly at the extremes of range, is essential in achieving pain-free movement. Improving posture and increasing range of movement in the joints of the neck, thoracic spine and ribcage plays a big role in managing this condition.
Once we get the basics under control it’s time to challenge the patient with higher level sport and work-related tasks such as lifting, pushing and pulling under load and at speed.
If you’re goal is to rebuild a dynamic highly functioning shoulder after experiencing an impingement syndrome then contact us and come and see one of our highly qualified physios today [ Click here to Request an Appointment ]
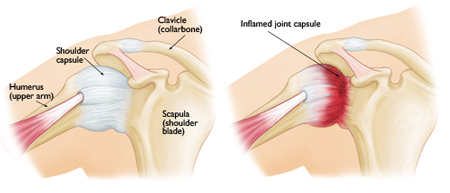
Frozen Shoulder
Frozen shoulder is a condition typified by pain and loss of movement of the shoulder joint and whilst we physios have a fancy name for it – adhesive capsulitis – we have a somewhat less impressive idea of why it happens. It seems to occur in some people following trauma or injury to the shoulder and in others it just seems to occur.
Risk Factors / Causes:
This is always going to be an incomplete list but includes: shoulder trauma; post-surgery or stroke; being female (sorry ladies); being 40-60 years old (sorry folks); diabetes; thyroid disease; connective tissue disorders; Parkinson’s disease and cardiac disease. As is always the case, from time-to-time we will have a patient walk through the door who fits none of these categories but still presents with a frozen shoulder.
Management:
Over time the symptoms of a frozen shoulder follow a fairly typical pattern:
Stage One (Freezing) – the patient notices a gradual onset of pain and restricted movement of the shoulder. These symptoms worsen over time and may last anywhere between six weeks and nine months.
Stage Two (Frozen) – fortunately pain is minimal during the frozen stage but the loss of movement remains. This last four to nine months.
Stage Three (Thawing) – I had a patient who preferred to refer to this as the Hallelujah Phase. Movement gradually returns over six to twelve months.
During Stage One (Freezing) we focus on pain management – gentle massage and joint mobilisation; taping for support; electrotherapy and acupuncture/dry-needling.
During Stage Two (Frozen) we focus upon slightly stronger mobilisation and tissue release techniques, whilst being careful not to aggravate the condition.
During Stage Three (Thawing) we focus upon restoring strength to the new-found range of motion. We also progress the techniques used during Stage Two to gain further joint movement and normal active range for a pain-free fully functional shoulder.
If you’re goal is to rebuild a dynamic highly functioning shoulder after experiencing frozen shoulder syndrome then contact us and come and see one of our highly qualified physios today [ Click here to Request an Appointment ]