When people speak of a fractured wrist they are usually referring to a fracture at the end of the long bone of the forearm known as the distal radius. This is known as a Colles’ Fracture. In actual fact any of the 10 bones (eight in the wrist and the two long forearm bones) that make up the wrist are subject to trauma-induced damage.
Risk Factors / Causes:
The most common cause of a wrist fracture is a fall onto the outstretched hand (FOOSH). It’s common in the active – through falls from bikes or skateboards and the like – and in the elderly due to loss of balance compounded by osteoporotic changes in the bone.
Management:
With a simple fracture the wrist is placed in a cast for up to six weeks after which physio may begin. In this case the primary goal of physio is to restore movement to the wrist and hand. We also help with secondary stiffness at the neck, shoulder and elbow due to wearing a sling or carrying a cast.
When a fracture requires surgery to stabilise the bone physio will begin on the day of or within several days of the operation. At first the physios role is to assist the patient to overcome the effects of the surgery. This is of particular importance where the patient is elderly and needs to get up and moving to help promote healing and prevent infection and other secondary disorders that can occur as a consequence of trauma, anaesthesia and immobilisation. We also work with the patient to regain movement of the fingers and promote pain management and fluid clearance. As healing continues we work with the patient to regain movement and strength of the wrist, fingers, elbow and shoulder joints.
If you’re recovering from a fractured wrist and need help with your rehabilitation then come and see one of our highly qualified physios today [ Click here to Request an Appointment ]
Chronic
Carpal Tunnel Syndrome – CTS
Carpal Tunnel Syndrome (CTS) is a painful disorder of the wrist and hand characterised by pain, pins and needles and numbness in the thumb and first two and part of the third finger. As the condition progresses weakness and muscle loss may eventuate.
Risk Factors / Causes:
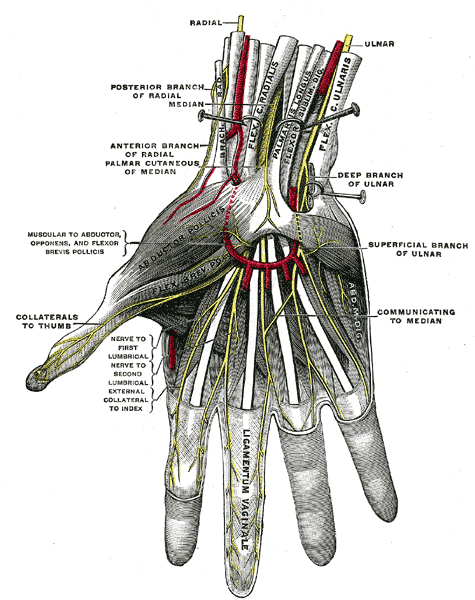
The Carpal Tunnel is a space in the wrist that has the wrist bones as its floor and a thick band of connective tissue, known as the flexor retinaculum, as its roof. Passing through this tunnel are the tendons, blood vessels and nerves that supply the hand and fingers. Chronic inflammation of the tendons/tendon sheaths or trauma to the wrist can narrow the tunnel leading to pressure, restriction or irritation of the median nerve leading to the classic CTS symptoms of numbness, pins and needles or pain.
CTS can also arise due to restriction of the median nerve at a point remote from the wrist. A bulging disc or other disorders of the lower cervical and upper thoracic spines can place pressure on the nerve tissue as it exits the spine causing a loss in the normal nerve function. This loss of normal function essentially ‘starves’ the nerve, leading some individuals to experience CTS symptoms. This is referred to as a “double crush syndrome”.
Those at risk of developing CTS are: workers who perform repetitive tasks (data entry clerks; painters; steel fixers) or use high impact or vibratory tools such as jack-hammers or rattle guns; pregnant or middle-aged women who experience swelling of the hands or wrist; and secondary to wrist trauma – significant soft or bony tissue damage following a fall or direct impact.
Management:
Many CTS sufferers benefit greatly from the use of a night splint to hold the wrist straight and lessen pressure build-up within the carpal tunnel. This along with avoidance of the task(s) that contributed to the development of CTS is a good first step.
A thorough assessment of the neck and upper-back is undertaken to screen for cervical or thoracic disc dysfunction that may contribute to a “double crush syndrome”. Where dysfunction is found, the physio will mobilise the joints, release tight tissue and give postural retraining and strengthening exercises to reduce the spinal contribution to CTS.
Nerve mobilisation exercises are given to ‘free-up’ the median nerve and improve its function.
The physio will mobilise the joints of the wrist and use massage and other tissue release techniques to improve mobility of the forearm and wrist.
Strengthening and mobility exercises are important for the long-term CTS sufferer who has experienced loss of motor function of the muscles of the hand.
In cases that are non-responsive to conservative management (rest, physio), surgery may be required. The general rule is to adopt conservative measures for 6-12 months after which if symptom resolution has not been achieved then we progress to surgery.
Post-op CTS rehab is very similar to that for conservative management – nerve and joint mobilisation (wrist and neck/upper back); soft and connective tissue release; night-splints; postural re-education; stretching and strengthening.
If you think you have CTS or are recovering from CTS surgery and need help with your rehabilitation then come and see one of our highly qualified physios today [ Click here to Request an Appointment ]
De Quervain’s Tenosynovitis – DQT
We’ll start with a brief anatomy class to explain this one. De Quervain’s Tenosynovitis, which to keep it simple we will refer to as DQT, is an inflammatory condition effecting the tenosynovium or sheath of two of the tendons that move the thumb. One of the tendons, the abductor pollicis longus (APL) is responsible for moving the thumb (pollicis) away (abduct) from the first finger. The other, the extensor pollicis brevis lifts the thumb. Irritation of these two structures leads to DQT. Symptoms of DQT are pain with gripping; tenderness at the base of the thumb and in some cases a “creaking” sound with side-to-side movement of the wrist.
Risk Factors / Causes:
DQT is usually an overuse injury due to repetitive loading of the tendons. I’ve seen it in electricians, steel-fixers, riggers and plumbers; in rock-climbers and have even experienced it myself courtesy of poor dip technique at the gym.
DQT can also present secondary to wrist trauma or as a consequence of arthritic conditions.
Management:
Physio management of DQT focuses upon pain control; muscle restrengthening; ergonomic advice; manual handling education and in some cases splinting or strapping to facilitate recovery.
If you think you have DQT and need help with your rehabilitation then come and see one of our highly qualified physios today [ Click here to Request an Appointment ]